Ebola does not wait for appropriations, procurement chains, or diplomatic reorganization. It moves through the delay.
Ebola does not wait for appropriations, procurement chains, or diplomatic reorganization. It moves through the delay.
By KOLUMN Magazine
In the first days of an Ebola outbreak, time is not measured only in hours. It is measured in gloves. In gowns. In test tubes. In trained contact tracers who can move before rumor does. In the distance between a fever in a mining town and a laboratory result that confirms what everyone fears.
That distance has become deadly in the Democratic Republic of the Congo.

By late May 2026, health authorities were confronting a fast-moving outbreak of Ebola disease caused by the Bundibugyo virus in eastern DRC and Uganda. The Centers for Disease Control and Prevention reported 906 suspected cases, 125 confirmed cases, 223 suspected deaths, and 17 confirmed deaths in DRC as of May 29, while Uganda had reported nine confirmed cases and two confirmed deaths. The World Health Organization warned that the number of suspected and confirmed cases had risen rapidly, spreading across Ituri, North Kivu, and South Kivu, with weak contact follow-up because of insecurity and movement restrictions.
The outbreak is not simply a virological event. It is a systems failure arriving in real time.
Unlike the Zaire ebolavirus strain that has shaped much of the public imagination around Ebola, the Bundibugyo virus currently has no licensed vaccine or specific approved treatment, leaving early detection, infection prevention, isolation, supportive care, and community trust as the main instruments of survival. Those instruments are precisely where the early warning signs have appeared: reported gaps in personal protective equipment, strained surveillance, limited testing access, and a frontline workforce asked to confront one of the world’s most feared pathogens without the full architecture that past outbreaks taught the world to build.
The outbreak began, as so many do, before the world had a name for it. WHO said retrospective investigations covering April 15 through May 13 identified suspected cases and deaths in Ituri before formal confirmation, while its May 17 emergency determination noted unusual clusters of community deaths, high early sample positivity, and healthcare-worker deaths suggesting gaps in infection prevention and control. The virus had been moving in the open, hidden inside symptoms that could look like malaria, typhoid, or any number of illnesses common in a fragile health setting.
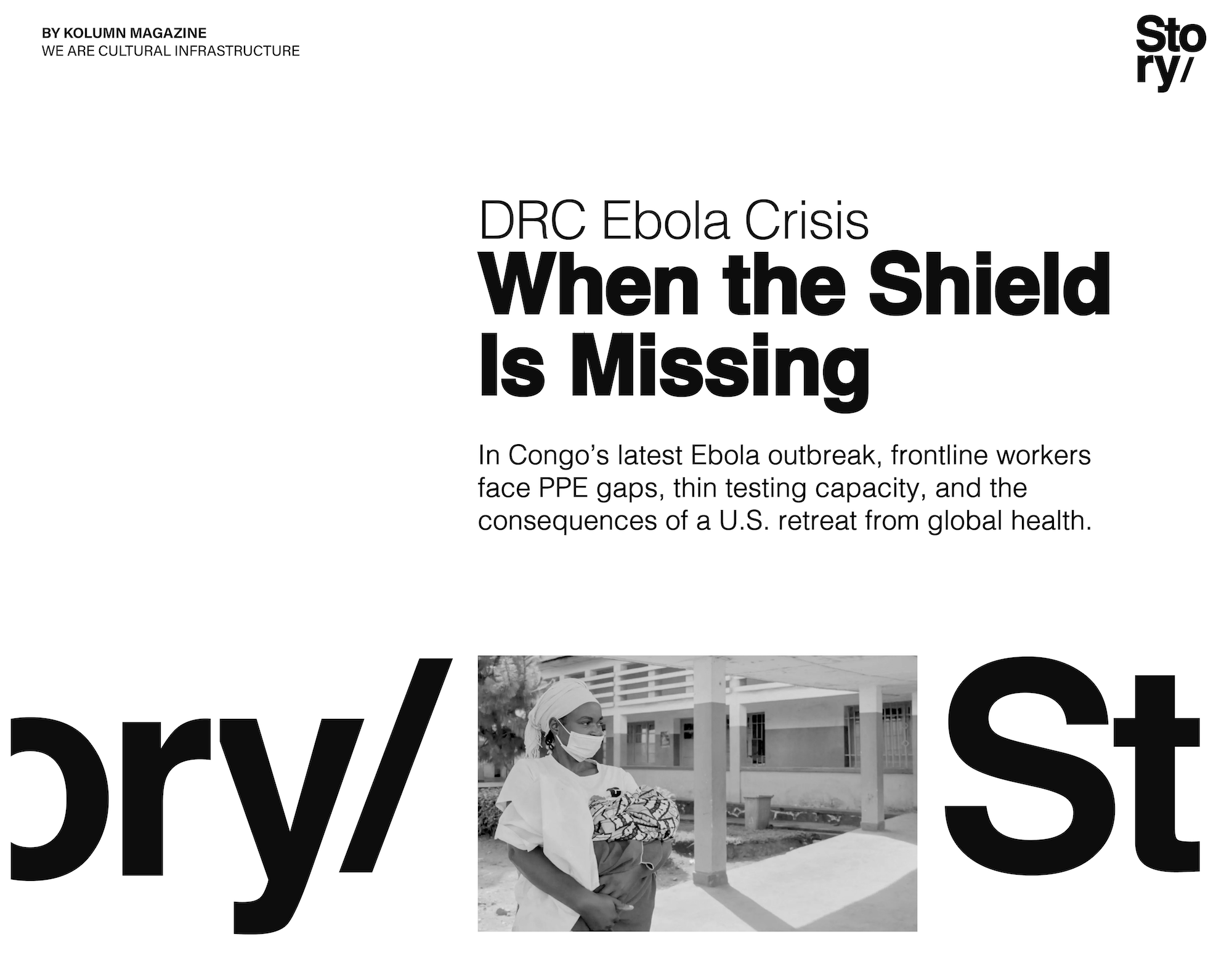
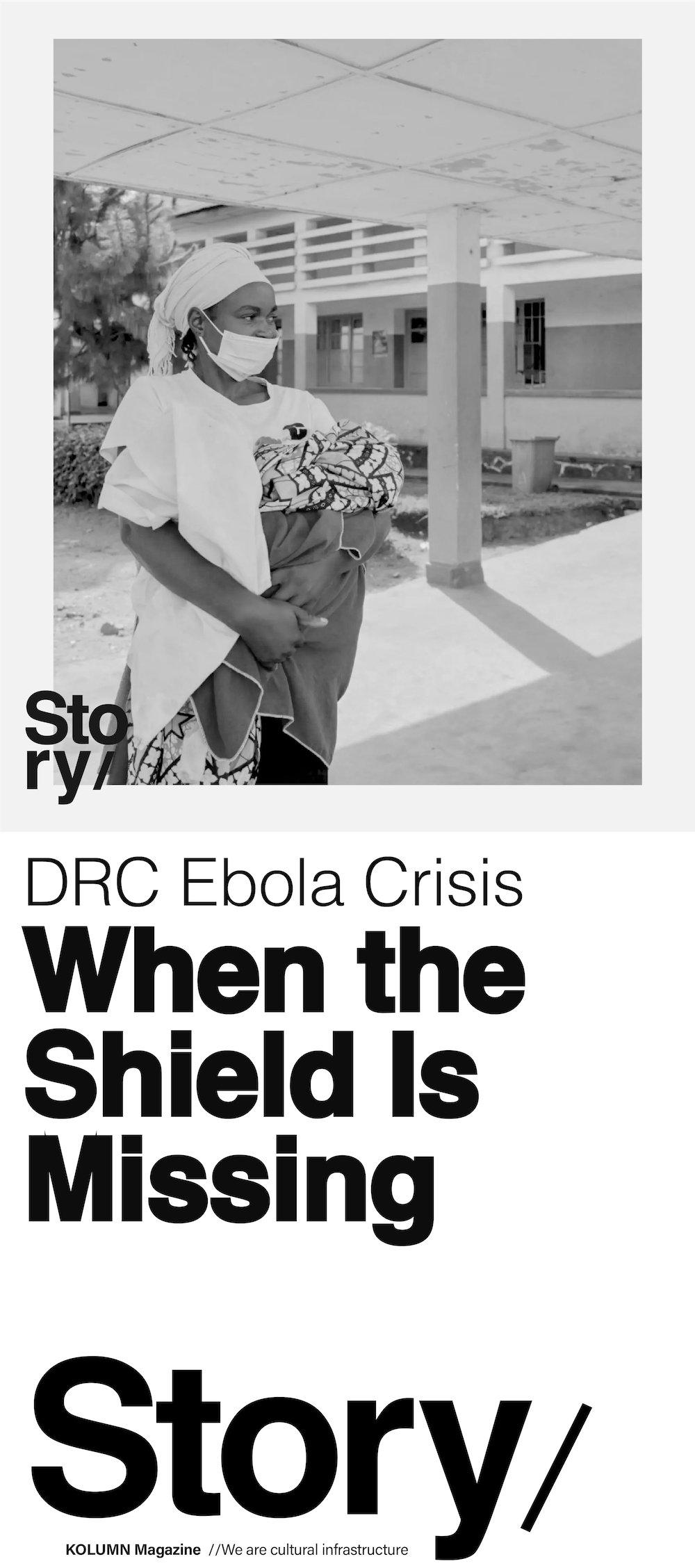
In Ituri, where mining camps, displacement, conflict, and poverty overlap, that ambiguity is dangerous. A fever is common. A laboratory is not always close. A safe burial protocol can sound like foreign intrusion. A protective gown may be the difference between a nurse going home and a hospital becoming an amplifier.
The first crisis was detection
The most urgent fact about Ebola is also the least cinematic: survival improves when people are identified early and treated quickly. The tragedy of delayed detection is that it robs patients and responders at the same time. Patients arrive late, already gravely ill. Health workers are exposed before they know they are treating Ebola. Contacts disperse before they can be traced. Rumors begin before public-health teams have earned trust.
In its emergency statement, WHO said early evidence pointed to a potentially larger outbreak than what was being detected and reported, citing the confirmation of cases in Uganda, the high positivity rate among initial samples, and syndromic reporting of suspected cases and deaths across Ituri. The agency also flagged healthcare-associated transmission as a concern after deaths among health workers in the affected area, an especially ominous sign in Ebola response because hospitals can become transmission nodes when protective systems fail.
Detection is never just a laboratory function. It is a chain: community alert, clinical suspicion, safe sample collection, protected transport, lab capacity, rapid communication, contact tracing, isolation, and public trust. Break any link and the virus gets time.
That chain appears to have been weakened before the outbreak was formally visible. STAT reported that U.S. aid reductions in the months before the outbreak probably hampered detection and response, citing six people involved in or familiar with public-health work in the region. Programs designed to detect Ebola cases, alert communities, and dispatch response kits had funding reduced or eliminated, according to that reporting. The International Rescue Committee said it had reduced programming from five to two areas at the heart of the outbreak after U.S. cuts, and IRC country director Heather Reoch Kerr warned that underinvestment and recent reductions had left facilities without adequate protective equipment, surveillance capacity, or frontline support.
These are not abstractions. A surveillance program is a person with a phone, a motorcycle, a relationship with a clinic, and enough fuel to follow a rumor. A response kit is the difference between improvisation and protocol. PPE is not a symbol of preparedness; it is preparedness, worn on the body.
The missing armor
The early public record shows both a shortage concern and a scramble to correct it. UNICEF USA reported that by May 18 it had mobilized nearly 50 tons of infection-prevention and control supplies, including disinfectants, soap, PPE, water-purification tablets, and water tanks to Bunia, the capital of Ituri province. A week later, UNICEF and the European Union announced more than 100 metric tonnes of additional emergency supplies, including medicines, infection-prevention items, PPE, tents, cholera and malaria treatment supplies, and equipment intended to support around 100,000 people.
That such shipments were necessary is itself revealing. In a fully prepared setting, PPE is pre-positioned near high-risk zones before the first confirmation. In this outbreak, major agencies were racing supplies into a region where health workers were already exposed, communities were already grieving, and case counts were already climbing.
The Guardian’s field reporting described the pressure on medical workers in Ituri, where health workers “can only do their jobs with a proper supply of PPE”, while Dr. Papys Lame, Ebola outbreak response coordinator in Ituri for ALIMA, emphasized that early care can improve a patient’s chance of survival even without a specific cure. In the same account, Lame described fear among patients and frontline workers, including colleagues who had died after treating patients.
Ebola punishes gaps in routine discipline. A glove removed incorrectly. A body washed according to family custom. A triage desk without masks and gowns. A nurse treating vomiting and fever before a test result returns. The virus turns scarcity into exposure.
That is why PPE shortages are never merely logistical. They reshape behavior. Health workers hesitate. Patients hide. Families resist isolation. Clinics become places of fear rather than care. In an outbreak zone, a missing box of gloves can become a missing layer of trust.
Trump’s cuts and the hollowing-out of response
The Trump administration’s approach to foreign aid and global health sits at the center of the current debate over responsibility. It is not accurate to say U.S. cuts alone caused the outbreak. Ebola emerges from complex ecological, social, and political conditions. Eastern DRC has endured war, displacement, weak infrastructure, resource extraction, and deep mistrust of state and foreign institutions. But it is equally inaccurate to pretend that funding cuts do not shape what happens after the first fever appears.
KFF’s policy analysis describes the current outbreak as the first major test of U.S. global outbreak response since the Trump administration’s restructuring of foreign assistance. It notes that the international environment has changed sharply because of U.S. withdrawal from WHO, reductions in foreign aid and health programming, and broader donor constraints. KFF also reported that the U.S. initially mobilized $23 million in emergency funding for DRC and Uganda, but that support is now operating through different mechanisms after the dissolution of USAID and the transfer of responsibilities to State Department structures with less operational experience in outbreak response.
That bureaucratic change matters. Epidemic response depends on institutional memory. USAID was not simply a bank account; it was a network of staff, implementing partners, procurement systems, emergency relationships, and field knowledge. When those systems are paused, dissolved, or reorganized, the loss is measured later in speed.
STAT reported that HHS foreign aid to DRC fell from nearly $33 million in fiscal 2024 to less than $10 million in fiscal 2025, while USAID funding also dropped sharply, with some figures subject to reporting lags. The same reporting described paused or canceled grants for public health, sanitation, infectious disease control, stockpiles, and local health systems. Those are precisely the categories that matter when Ebola returns.
The Trump administration has defended its response by pointing to new emergency funding, CDC support, and U.S. efforts to protect Americans in the region. That context belongs in the record. The U.S. has not been absent from the response. The CDC says it is responding to the outbreak and assessing U.S. risk as low. KFF noted that the U.S. has begun supporting partner organizations in procuring and deploying supplies, including PPE, and that CDC emergency operations have been activated.
But a late ramp-up does not erase an earlier hollowing-out. Outbreak systems are not built at the moment of alarm. They are built in the quiet months when donors lose interest.
Ebola: from colonial naming to global panic
To understand why this outbreak carries such weight, it helps to remember the long history of Ebola as both disease and narrative.
Ebola was first identified in 1976, in outbreaks in what is now South Sudan and in Zaire, now the Democratic Republic of the Congo. The virus was named after the Ebola River, a geographic choice that helped avoid attaching stigma to a specific village but still embedded the disease in the Western imagination as something remote, African, and terrifying. For decades, outbreaks were treated as episodic emergencies — deadly, dramatic, geographically contained — rather than as warnings about weak health systems, extractive economies, and global neglect.
The 2014–2016 West African epidemic changed that understanding. WHO notes that the West African outbreak was the largest and most complex Ebola outbreak since the virus was discovered, with more cases and deaths than all previous outbreaks combined. The epidemic exposed the cost of delayed international response, weak surveillance, fragile health systems, and public distrust. It also produced reforms: emergency funds, vaccine development, stronger coordination mechanisms, and a new appreciation for community engagement.
DRC then became the center of another major chapter. The 2018–2020 eastern Congo outbreak unfolded amid violence and mistrust, killing more than 2,000 people and testing the limits of modern Ebola response. It also demonstrated the promise of biomedical advances, including vaccines and therapeutic trials for Zaire ebolavirus. But the current Bundibugyo outbreak is a reminder that science does not advance evenly across viral species. Preparedness for one strain does not automatically solve another.
The historiography of Ebola is therefore not only medical. It is political. Each outbreak becomes an archive of what the world chose to build after the last one — and what it allowed to decay.
KOLUMN Magazine has consistently treated Black life, public memory, and institutional power as inseparable. In previously published KOLUMN work on public-health inequity, environmental harm, and state abandonment, the pattern is familiar: crisis is often framed as sudden only because the slow violence before it was ignored. The DRC outbreak belongs in that lineage. It is not only about a virus crossing bodies. It is about what happens when Black communities in the Global South are expected to absorb the first shock of a global threat with fewer tools than the world knows how to provide.
Expert voices and the politics of preparedness
The expert consensus emerging around this outbreak is not that one donor can stop Ebola alone. It is that preparedness is cumulative and fragile. Cut it, and the damage appears later.
Dr. Papys Lame’s comments to The Guardian capture the clinical reality: even without a specific treatment, early presentation can save lives. But patients often arrive late because they fear isolation, mistrust health systems, or mistake symptoms for more familiar illnesses. That is where community health workers matter. They interpret the public-health system for families and interpret community fear for responders.
Megan Coffee, a senior infectious disease specialist at the International Rescue Committee, told STAT the region faced a “perfect storm,” shaped by migrant labor around mines, conflict-driven displacement, and aid cuts that weakened the health system. That analysis is crucial because it refuses the false separation between health and politics. An outbreak in a stable, well-supplied health system behaves differently from an outbreak in a conflict zone where facilities lack PPE, surveillance is thin, and communities have reasons to distrust outsiders.
KFF’s analysis adds the policy architecture: the U.S. response is being attempted after USAID’s dismantling, through newer State Department mechanisms and under the shadow of U.S. withdrawal from WHO. That does not mean coordination is impossible. It means the system is being tested under self-imposed constraints.
Public-health preparedness is often invisible when it works. There is no headline for a case detected early, a cluster contained, a nurse protected, a rumor answered before it becomes a riot. The danger of austerity is that it mistakes invisibility for dispensability.
Conflict, mistrust, and the burden on Congolese communities
The affected region is not an empty map on which international agencies operate. It is home to communities already living through violence, displacement, poverty, and political abandonment. WHO has warned that insecurity and movement restrictions are weakening contact follow-up. The Guardian reported attacks on health facilities and resistance to safe burials, including anger after the death of a young footballer suspected of Ebola.
These dynamics are often described as “community resistance,” but that phrase can flatten history. People resist when they are afraid. They resist when institutions arrive only in emergencies. They resist when burial rites are interrupted by strangers wearing protective suits. They resist when global systems seem more interested in containment than care.
That does not make unsafe practices harmless. Ebola can spread through contact with bodies after death, making safe burial essential. But public health cannot rely on command alone. It needs legitimacy, and legitimacy is built before outbreaks.
The same is true of health-worker safety. Nurses, doctors, cleaners, ambulance drivers, burial teams, laboratory staff, and community mobilizers carry the physical risk of the response. When PPE is scarce, they are asked to perform courage in place of infrastructure. When colleagues die, fear spreads inside the very workforce needed to stop transmission.
A global response still catching up
The international response is now accelerating. UNICEF and the EU are flying in emergency supplies. WHO has mobilized emergency funding and leadership. CDC is active. The U.S. has pledged support. MSF has announced preparations for a large-scale response in DRC through its Doctors Without Borders update. Regional authorities are coordinating across borders.
But Ebola response is unforgiving. The question is not whether the world can eventually mobilize. It is whether it can mobilize before the outbreak outruns the map.
By May 21, WHO said 1,603 contacts had been listed in Ituri, but follow-up remained weak, with a follow-up rate of 21 percent. That figure is the quiet alarm inside the louder case counts. Contact tracing is how Ebola’s future is interrupted. If contacts are not followed, the virus writes the next chapter.
There is also a biomedical gap. For Zaire ebolavirus, the world has vaccines and treatments that changed the response landscape. For Bundibugyo virus, no licensed vaccine or specific treatment exists, though WHO says work is underway to test promising candidates. This means old-fashioned outbreak control remains essential: surveillance, PPE, isolation, infection prevention, safe burials, and trust.
What accountability requires
The ethical question is not only what the Trump administration is doing now. It is what was dismantled before now.
A fair account must recognize multiple truths. Eastern DRC’s outbreak environment is extraordinarily difficult. Congolese authorities, local health workers, African public-health institutions, WHO, UNICEF, MSF, IRC, ALIMA, and others are operating under conditions most wealthy countries would struggle to manage. The U.S. has provided emergency support. No single donor owns the entire response.
But the record also shows that U.S. funding cuts and institutional disruption weakened epidemic preparedness in the region before the outbreak was fully detected. They reduced staff, interrupted programs, damaged supply chains, and forced organizations to shrink their footprint. When Ebola arrived, the system had less armor.
That is the accountability line: not that Washington created the virus, but that policy choices helped determine how exposed people were when the virus appeared.
The outbreak after the cuts
The DRC has lived with Ebola longer than any nation should have to. Its scientists, clinicians, and communities have contributed enormously to the world’s knowledge of the disease. Yet each outbreak seems to require Congolese people to prove again that their lives are worth urgent global investment.
The current crisis is a test of whether the world remembers what it learned. It is a test of whether wealthy governments understand that global health security cannot be turned on like a switch after being cut like a line item. It is a test of whether frontline workers in Ituri will receive what they need before they become statistics in another emergency report.
Ebola thrives in delay. It exploits silence, scarcity, distrust, and distance. The antidote is not only medicine. It is preparation. It is PPE already in place. It is testing close enough to matter. It is a surveillance worker whose job was not eliminated. It is a community liaison who speaks the language of fear before fear becomes refusal. It is a donor government that understands that the first mile of outbreak response may be in Congo, but the consequences are never local for long.
In the end, this outbreak is not just asking whether the world can stop Ebola. It is asking whether the world can stop repeating itself.
More great stories
Afro Sheen, Wall Street, and the Architecture of Black Possibility
July 6, 2026
No Comments
The Fire Inside the Fourth
July 5, 2026
No Comments