Before Williams entered medical history through the chest of James Cornish, he had already performed a different kind of surgery: he cut into the architecture of exclusion.

Before Williams entered medical history through the chest of James Cornish, he had already performed a different kind of surgery: he cut into the architecture of exclusion.
By KOLUMN Magazine
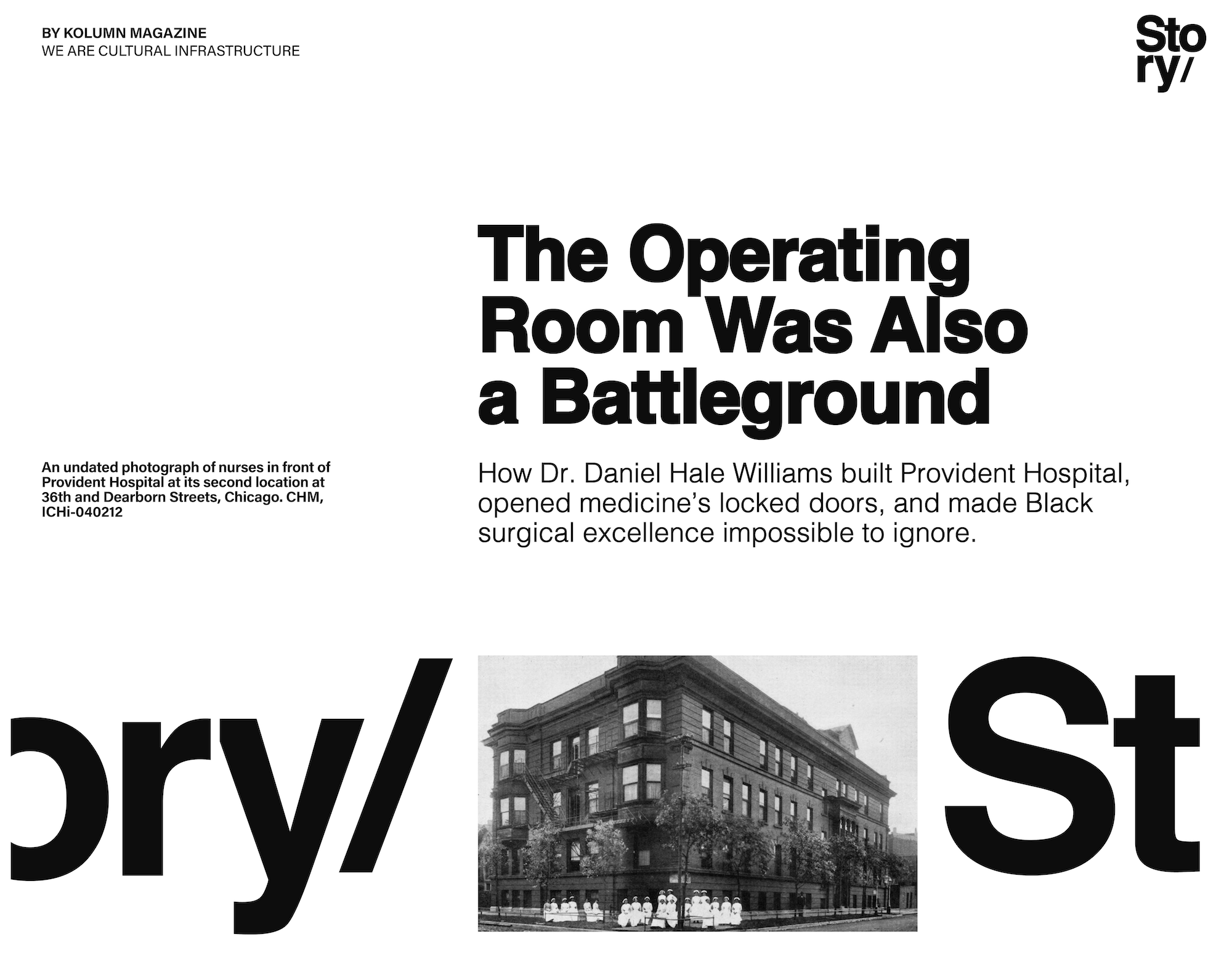
In the mythology of American medicine, Dr. Daniel Hale Williams is often introduced at the most dramatic possible moment: Chicago, July 1893, a wounded man on an operating table, a knife injury near the heart, a surgeon working without X-rays, antibiotics, blood banking or the modern architecture of cardiac care. The patient, James Cornish, had been stabbed in the chest. Williams opened the wound, repaired the pericardium—the protective sac around the heart—and Cornish survived. The story has been told for generations as one of the first successful operations involving the human heart, and the National Library of Medicine identifies Williams as a leading surgeon, educator and founder of Provident Hospital and Training School in Chicago.

But to begin and end with the operation is to reduce Williams to a heroic scene and miss the larger architecture of his life. His most enduring intervention may not have been the incision. It may have been the institution.
Provident Hospital, opened in 1891, was born out of a brutal ordinary fact: Black Chicagoans were blocked from the training, employment and care that white medical institutions controlled. Emma Reynolds, a Black woman who wanted to become a nurse, was rejected by Chicago nursing schools because of her race; her brother, the Rev. Louis Reynolds, turned to Williams for help, and the appeal became the seed of a hospital and nursing school built to answer exclusion with capacity, not simply complaint. The Chicago History Museum recounts that Williams first tried to persuade existing programs to admit Emma Reynolds before joining with community leaders to build something new.
“Provident was not charity dressed as medicine. It was a Black-led institution claiming the right to train, heal, govern and innovate.”
That distinction matters. Provident was not only a refuge from discrimination. It was a rebuttal to it. The hospital treated Black and white patients, assembled an interracial staff, trained Black nurses and gave Black physicians access to hospital practice at a time when most white institutions shut them out. The Encyclopedia of Chicago notes that Williams organized Provident Hospital and Training School in 1891 as a response to the exclusion of Black medical professionals from Chicago’s hospitals. The Library of Congress describes Provident as the first Black-owned and operated public hospital and medical training facility in the United States.
For KOLUMN readers, the story sits beside earlier magazine recoveries of Black medical infrastructure, including KOLUMN’s piece on Freedom House, the Pittsburgh ambulance service where Black paramedics helped define modern emergency medicine, and KOLUMN’s reporting on Henrietta Lacks, which examined how Black patients moved through segregated medical systems that extracted from them even as they denied them power. Provident belongs in that same lineage: not as a sentimental landmark, but as infrastructure made under pressure.
The Chicago That Needed Provident
Daniel Hale Williams was born in Hollidaysburg, Pennsylvania, in 1856, according to Britannica’s biography, though some older accounts have used 1858. He trained at Chicago Medical College, now associated with Northwestern University’s medical lineage, and graduated in 1883. Northwestern’s Galter Health Sciences Library describes him as the medical school’s first African American graduate and notes that he later served as an instructor, became surgeon-in-chief at Freedmen’s Hospital in Washington, D.C., and helped found the National Medical Association.
Chicago in Williams’s professional lifetime was a city of explosive growth and hardening racial boundaries. Black migration to the city was increasing, but the institutional pathways into medicine remained narrow. Hospitals were not merely places of healing; they were gateways into legitimacy. A physician who could not secure hospital privileges could be kept from surgery, teaching, clinical advancement and professional authority. A nurse denied admission to training was not simply denied a classroom. She was denied a profession.
“The first patient Provident treated was not only a person in a bed. It was the wounded idea that medicine belonged to white institutions alone.”
Williams understood the structural nature of the problem. The story of Emma Reynolds is often told as if one racist rejection produced one heroic institutional response. The deeper truth is sharper: Reynolds’s rejection exposed an entire medical order. If Black women could not train as nurses, Black physicians could not gain privileges and Black patients could not assume dignified access, then medicine itself was functioning as a racial gatekeeping system.
The founding of Provident answered that system with a different model. The Provident Foundation’s history states that Reynolds was denied admission by Chicago nursing schools because she was Black, after which Williams and community leaders moved toward creating a nursing school for Black women. WTTW’s account of early Chicago history likewise frames Provident as a direct response to Black doctors’ limited access to white hospitals and Black women’s exclusion from nursing education.
Provident’s interracial character was also radical. It did not simply reverse segregation by building a Black-only space. It built a Black-led space that refused the racial logic of the institutions that had made it necessary. The hospital was interracial in staff and patient care, and that fact carried both symbolic and practical force. It asserted that Black leadership and interracial excellence were not contradictions. They were the future medicine claimed to want but refused to organize.
A Hospital as a Civil Rights Argument
To call Provident a hospital is accurate. To call it only a hospital is insufficient.
It was a medical schoolhouse, a clinical proving ground, a civic project, a race-relations experiment and a political argument in brick and policy. Historian Vanessa Northington Gamble has written extensively on Black hospitals and medical segregation, and her landmark scholarship, including work on Provident, places institutions like it inside the broader struggle over Black professional autonomy and patient care. Her article “The Provident Hospital Project: An Experiment in Race Relations and Medical Education,” cited in medical historical discussions of Williams, helped move the subject beyond hero biography and into institutional analysis.
That historiographical shift is crucial. For much of the 20th century, Williams was celebrated in what might be called the “great man” frame: the brilliant Black surgeon who performed a daring heart operation. That frame was not false, but it was incomplete. It made Williams exceptional without fully explaining the system that required his exceptionalism. Later historians of Black medicine have complicated the story by asking different questions: Who funded Provident? Who governed it? How did Black nurses experience the institution? What did interracial staffing mean in practice? How did Black hospitals both resist and operate within segregated health care?
The Journal of the National Medical Association’s archived material on Provident preserves the way Black medical professionals themselves narrated the hospital’s significance across generations. In those accounts, Provident was not merely a memorial to Williams. It was a working institution whose meaning changed as Black medical access changed.
The hospital also belongs to the larger Black hospital movement. Across the United States, Black physicians and communities built hospitals because mainstream institutions excluded them as practitioners, humiliated them as patients or both. These hospitals were often underfunded and overburdened, but they performed indispensable work. They trained nurses, gave physicians surgical experience, protected Black patients from hostile treatment and cultivated professional networks that white medicine refused to provide.
Provident’s early success gave the movement a powerful example. It showed that a Black-led hospital could maintain standards, attract interracial support and produce medical excellence. It also exposed a recurring American hypocrisy: Black institutions were often required to prove excellence under conditions white institutions never had to survive.
The Operation That Became Legend
The 1893 operation remains central to Williams’s reputation for good reason. Cornish arrived at Provident with a stab wound to the chest. Williams operated at a time when cardiac surgery was widely considered dangerous, even taboo. The modern surgical world of intensive care units, heart-lung machines, blood typing, antibiotics, advanced imaging and cardiothoracic specialization did not yet exist. Williams relied on anatomical knowledge, surgical judgment, antiseptic technique and nerve.
The American Heart Association’s account places the operation in the context of Williams’s broader medical legacy, emphasizing both the surgical achievement and the founding of Provident as a Black-owned and operated hospital treating Black and white patients. Columbia Surgery’s historical overview similarly describes Williams as a pioneer whose 1893 operation became one of the landmark moments in early heart surgery.
Still, accuracy requires care. Popular accounts often state that Williams performed “the first successful open-heart surgery.” Historians and surgeons have debated that phrasing. Some earlier pericardial operations occurred before Williams, and later cardiac surgery histories distinguish between operations on the pericardium, the heart itself and procedures performed under direct visualization inside the heart. A 1984 article in The Annals of Thoracic Surgery, “In Proper Perspective: Daniel Hale Williams, M.D.,” underscores the need to place Williams’s work accurately within the early evolution of cardiac surgery rather than flattening it into a slogan.
That does not diminish Williams. It sharpens him. The better formulation is that Williams performed one of the first successful operations involving the heart region in the United States, successfully suturing a pericardial wound at Provident Hospital. The operation was daring, consequential and historically important, especially because it occurred inside a Black-founded hospital whose very existence challenged medical segregation.
In 1897, Williams reported the case in Medical Record under the title “Stab Wound of the Heart and Pericardium—Suture of the Pericardium—Recovery—Patient Alive Three Years Afterward,” a title cited in later medical scholarship, including Alpha Omega Alpha’s profile of Williams. That delayed publication matters. It reminds us that historical recognition is often not immediate, especially for Black innovators whose work had to travel through professional systems not built to honor them.
Williams at Freedmen’s Hospital
Williams’s significance widened after Provident. In 1893, President Grover Cleveland appointed him surgeon-in-chief at Freedmen’s Hospital in Washington, D.C., the major institution serving Black patients in the nation’s capital. The National Library of Medicine notes that Williams served there and also taught at Howard University’s medical department.
Freedmen’s Hospital carried its own symbolic weight. Born in the aftermath of the Civil War, it was tied to the federal government’s response to formerly enslaved people and the health needs of Black Washington. By the time Williams arrived, it was a hospital, a teaching institution and a battleground over standards, authority and racial politics. His role there extended his institutional philosophy: Black patients deserved high-quality care, and Black medical professionals deserved rigorous training and leadership authority.
Williams’s administrative work is less cinematic than the Cornish operation, but it may tell us more about his mind. He was not simply a surgeon who wanted to operate. He was a system-builder who wanted medicine organized differently. That meant standards. It meant training. It meant discipline. It meant Black physicians and nurses entering the profession not as tokens of benevolence but as competent practitioners backed by institutions.
This is where Williams’s story also intersects with the founding of the National Medical Association in 1895. The NMA emerged because Black physicians were often excluded from the American Medical Association and other professional bodies. Williams was among the founders, and the organization became a crucial vehicle for Black medical advocacy. The National Medical Association’s own history explains that it was created when Black physicians were denied membership and participation in mainstream medical organizations.
In this light, Provident, Freedmen’s and the NMA form a trilogy: hospital, federal teaching institution, professional association. Williams’s career moved across all three. He was not only trying to heal patients. He was helping build the institutional ecology Black medicine needed to survive.
The Black Nurse at the Center of the Story
Emma Reynolds should not disappear into the origin story. Too often, she is treated as the woman whose exclusion inspired Williams’s action, then vanishes from the narrative once the hospital opens. But Reynolds’s aspiration matters. Provident began because a Black woman wanted professional training. Her ambition was not incidental. It was the spark.
Northwestern Medicine’s profile of Reynolds describes her as a woman who had long wanted to be a nurse and who later graduated from Provident’s nursing program before becoming a physician herself. In 1895, Emma Ann Reynolds became the first Black woman to earn a medical degree from Northwestern University Woman’s Medical School, a fact Northwestern Medicine highlights in its account of her life and legacy.
That trajectory transforms the Provident story. Reynolds was not merely denied opportunity. She became evidence of what opportunity could produce. Her path from rejected applicant to nurse to physician demonstrates why exclusion was so destructive: it did not protect standards; it wasted talent.
Provident’s nursing school was therefore not a side project. It was central to the institution’s mission. Black nurses were essential to Black health care, but nursing was also one of the professions through which Black women claimed public authority in an era that tried to confine them to domestic service or moral uplift without professional power. The Chicago History Museum’s essay on the Black nurses of Provident makes clear that the hospital’s training work was inseparable from the fight against racial exclusion in medical education.
This is where the article’s historiography must widen beyond Williams. Provident was built by a network: Williams, Reynolds, Rev. Louis Reynolds, Black clubwomen, church leaders, donors, physicians, nurses and patients. Heroic biography can obscure that collective labor. Institutional history restores it.
Race, Reputation and the Burden of Proof
Provident was frequently required to demonstrate what white institutions assumed: competence. Black hospitals operated under punishing conditions. They needed money, equipment, staff, political legitimacy and public trust. They also had to navigate white philanthropy without surrendering Black purpose.
This tension ran through many Black institutions of the late 19th and early 20th centuries. They needed interracial support but not paternalistic control. They needed credibility in white professional circles but not dependence on white approval. They needed to train Black professionals while resisting the segregated logic that made separate institutions necessary.
Williams was careful about standards because he knew standards could be weaponized. If Provident failed, racists would not call it an underfunded hospital. They would call it proof. If it succeeded, they might still call it exceptional. That is the trap Black institutions have long faced: failure is generalized; success is isolated.
The hospital’s interracial staff was one way Provident challenged that trap. It asserted that Black leadership could organize across race without submitting to white control. It also gave white physicians an opportunity to participate in a different kind of medical institution, though the moral burden remained clear: Provident existed because white institutions had failed.
There is a modern echo here. KOLUMN’s “The White Coat Threshold” examined the slow and uneven progress of Black representation in medical education. Williams’s world and ours are not the same, but the structural question persists: Who gets trained? Who gets trusted? Who gets institutional backing? Who gets remembered as a pioneer, and who gets treated as a beneficiary?
Provident’s Afterlife
Provident’s history did not end with Williams. The hospital moved, expanded, struggled, closed and was revived under changing political and health-care conditions. The Encyclopedia of Chicago traces Provident’s long arc from its founding through its later institutional transformations. Cook County Health now identifies Provident Hospital as part of its system and has commemorated its modern anniversary, noting the institution’s roots in Williams’s response to discrimination.
That afterlife matters because Black institutions are often remembered only at the moment of founding or crisis. But institutions live in maintenance. They require budgets, boards, staff, repairs, reinvention and public support. Provident’s survival as memory and facility reflects both the power and fragility of Black medical institution-building.
The Black hospital movement itself was transformed by desegregation and federal health policy. As white hospitals opened under legal and financial pressure, many Black hospitals lost patients, staff and funding. Integration, in theory, promised access. In practice, it sometimes weakened Black-controlled institutions without fully eliminating disparities in care. This is one of the central paradoxes historians of Black health care have explored: the end of formal segregation did not automatically preserve Black medical autonomy.
Provident therefore forces a more complicated question than “Was integration good?” The question is: What happens when institutions built by excluded people become vulnerable once the dominant system partially opens? What is gained when doors open? What is lost when Black-governed institutions lose their base? What forms of power can be preserved?
The Meaning of Williams Now
Daniel Hale Williams died in 1931 in Idlewild, Michigan, a Black resort community that itself represents another form of Black institution-building. By then, his legacy had already entered the realm of medical memory. He had been a surgeon, hospital founder, educator, administrator and professional organizer. He had made history in the operating room, but he had also made history before the incision, when he helped turn a rejected Black nursing applicant’s frustration into a hospital.
The reason Williams still matters is not simply that he was first, though firsts have their place. He matters because he exposed the lie behind exclusion. Black people were not absent from medicine because they lacked talent. They were kept from medicine because institutions guarded opportunity. When Williams built Provident, he did not beg the old system to become kind. He created a new threshold.
His story also cautions against shallow celebration. It is easy to put Williams on a poster during Black History Month and call the work done. It is harder to confront the conditions that made Provident necessary. It is harder to ask why Black patients still experience disparities in treatment, why Black physicians remain underrepresented in many specialties, why community hospitals serving Black neighborhoods are often financially endangered, and why medical innovation is still remembered unevenly.
Williams’s life belongs to a lineage that includes Charles Drew, whose blood-plasma research KOLUMN has previously summarized in its profile of Drew; Alice Ball, whose scientific breakthrough KOLUMN examined in “Alice Ball’s Cure, and the Theft That Followed”; and Freedom House, whose Black medics helped modernize emergency care. These stories differ, but they share a pattern: Black excellence emerges, institutions resist or exploit it, and history later struggles to decide whether to honor the person without indicting the system.
The Door He Left Open
Provident Hospital began with refusal. A woman was told no. A physician saw that the no was larger than one school. A community built an answer.
That is the lasting significance of Daniel Hale Williams and Provident Hospital. They remind us that access is not an abstraction. It is a bed, a classroom, an operating room, a staff appointment, a chart, a diploma, a patient who survives. It is also governance—the power to decide who belongs inside the institution and what standards will mean.
Williams’s operating-room triumph deserves its place in history. But the greater achievement was the world around that room: a Black-founded, interracial hospital that trained nurses, elevated physicians and proved that medicine could be practiced against the grain of American racism. Provident was not perfect. No institution is. But it was profound because it understood that health care is never only about treatment. It is about power.
In the end, the most important thing Williams sutured may not have been the pericardium. It may have been the torn relationship between Black aspiration and American medicine—stitched under pressure, against the odds, in a hospital built because someone refused to accept that the door was closed.
More great stories
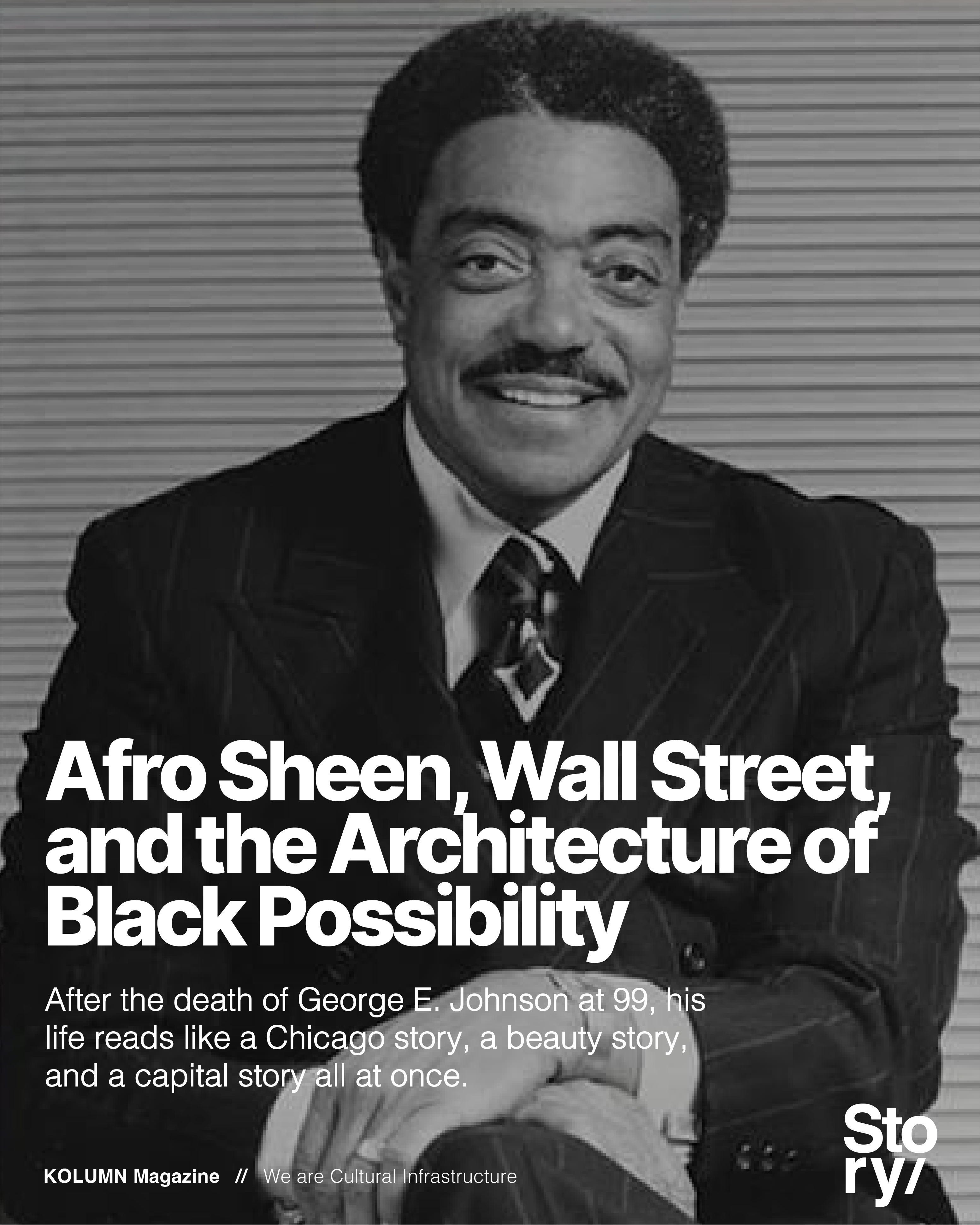
Afro Sheen, Wall Street, and the Architecture of Black Possibility
July 6, 2026
No Comments
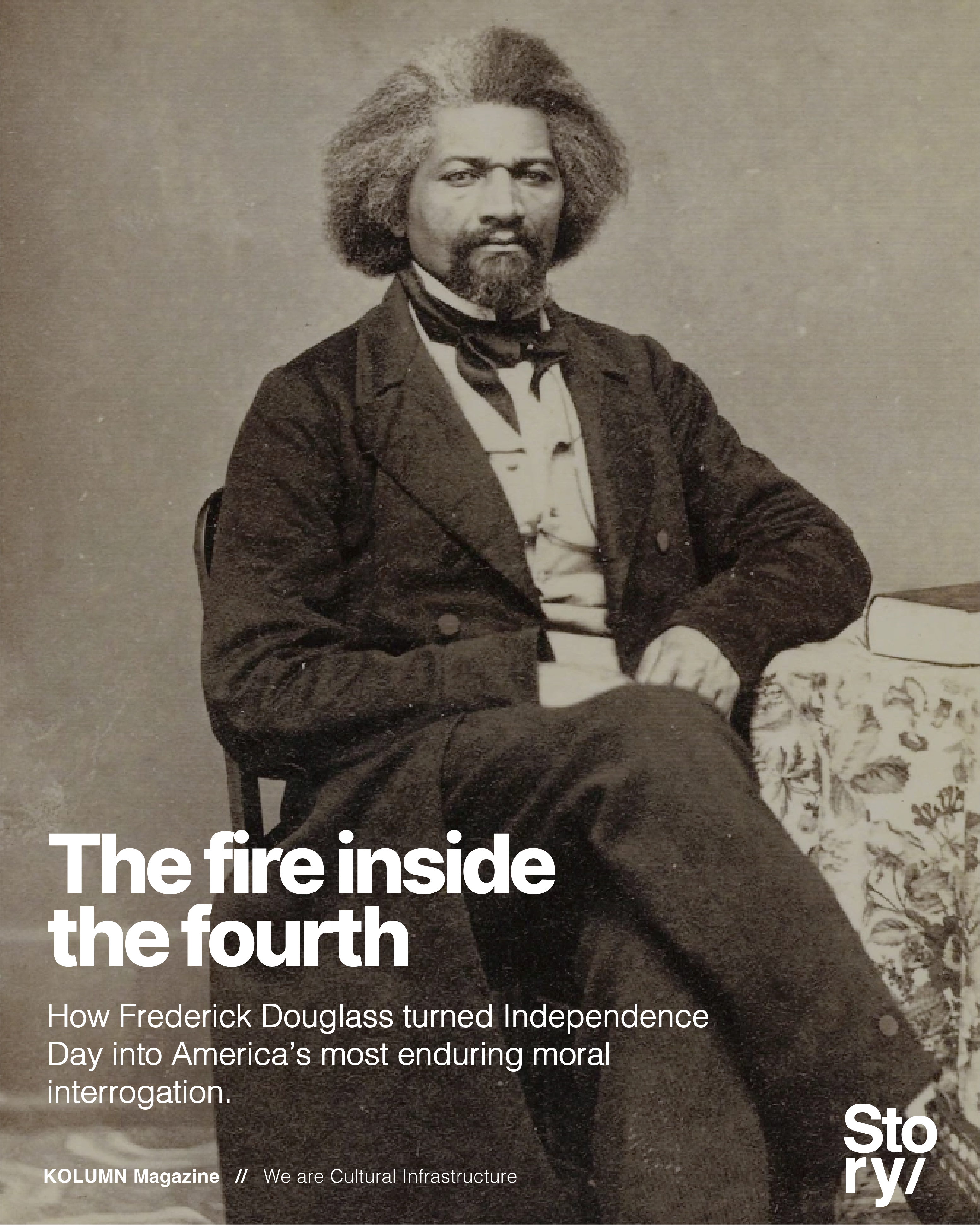
The Fire Inside the Fourth
July 5, 2026
No Comments