When the people you’ve overlooked build the future anyway, what do you owe them besides applause?
When the people you’ve overlooked build the future anyway, what do you owe them besides applause?
By KOLUMN Magazine
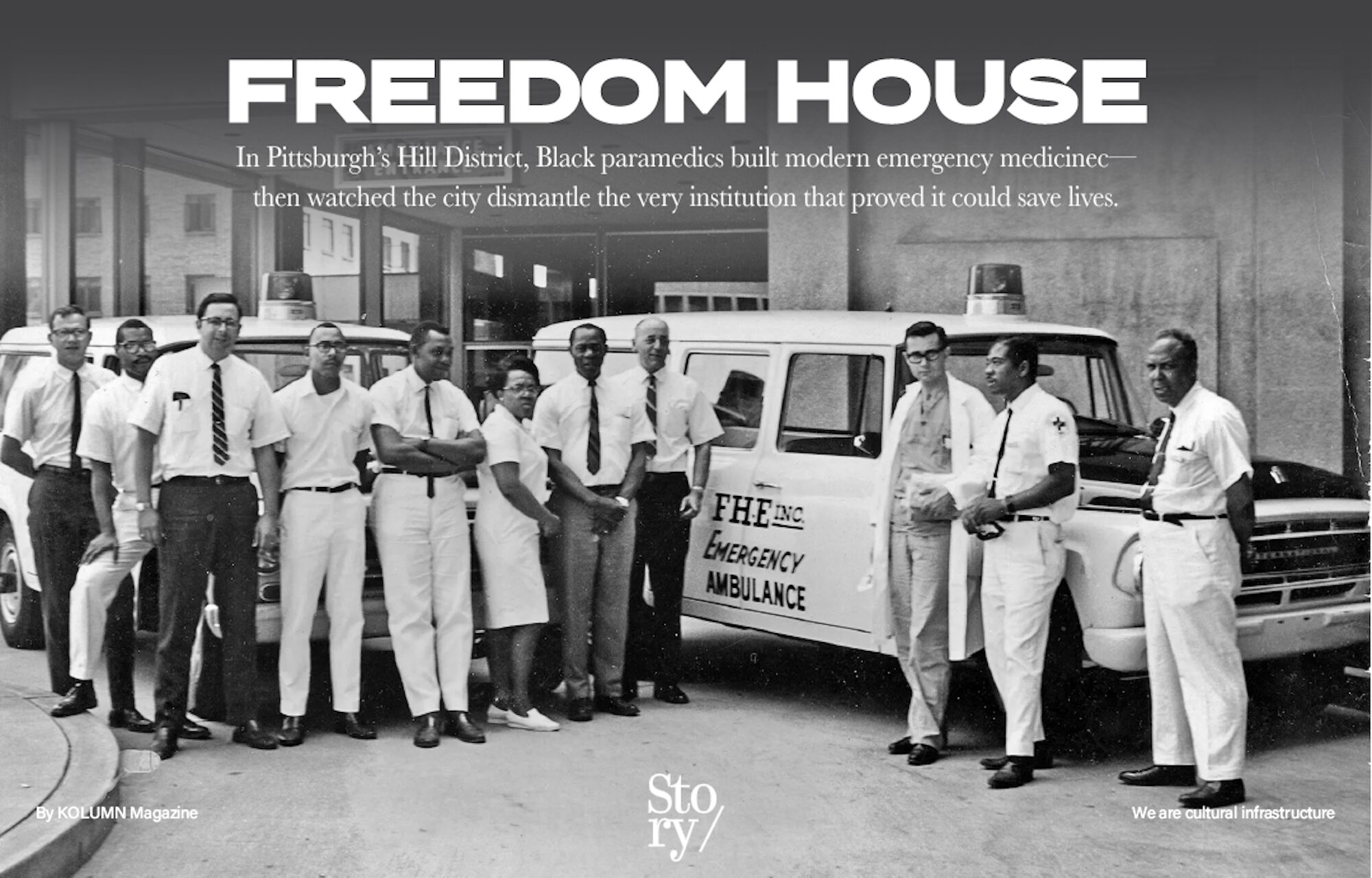
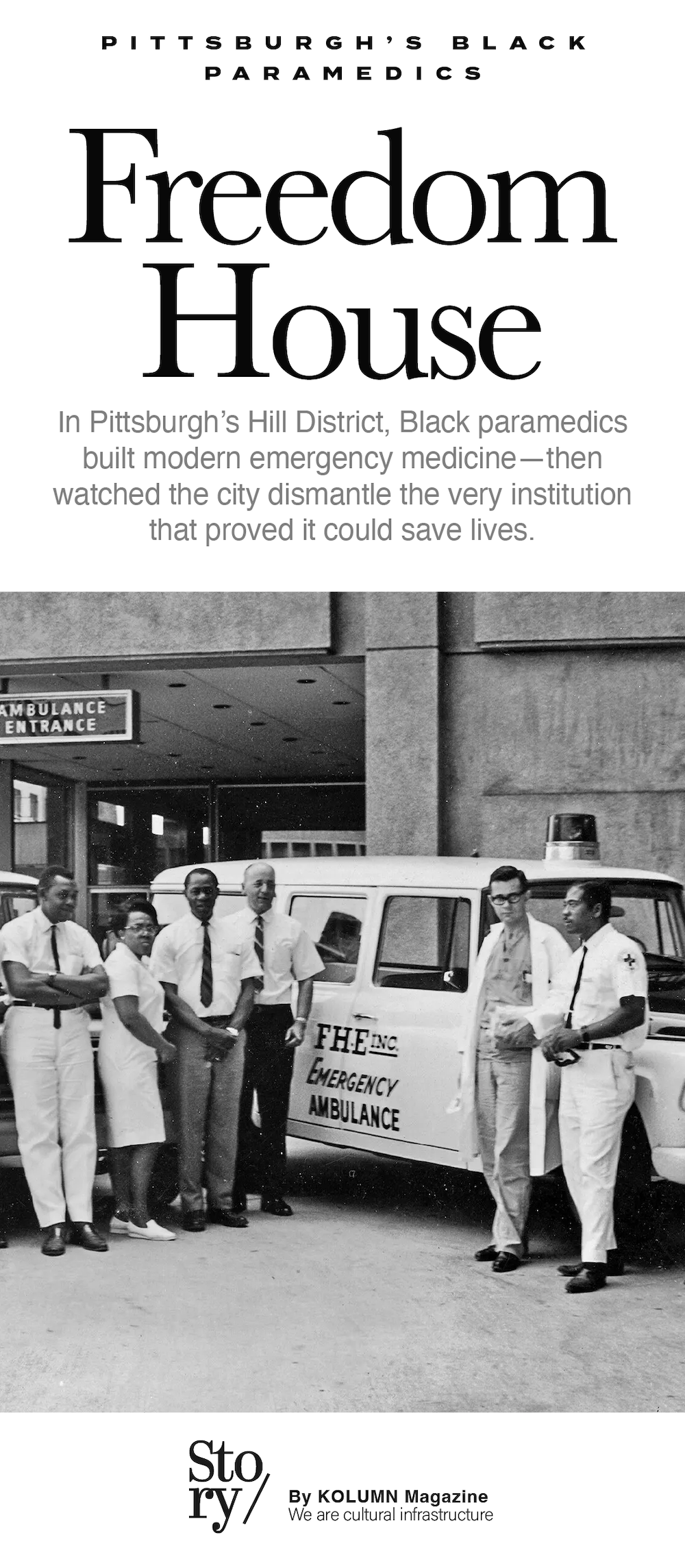
If you want to understand how modern emergency medicine became something more than speed and luck—how it became a disciplined practice capable of saving a patient before the hospital doors swing open—you eventually end up in Pittsburgh’s Hill District, in the late 1960s, listening for a dispatch call that residents learned to say like a prayer: Send Freedom House.
The phrase is memorable partly because it’s so plain. It’s not a brand slogan or a political chant. It is a request for competence, voiced by people who had learned through experience that emergency response was not distributed equally across a city. In the Hill, the arrival of help had long been uncertain, sometimes late, and too often intertwined with policing. Freedom House was different. It offered clinical skill where there had been improvisation, and it offered care where there had been suspicion. It turned an ambulance—once, in many American cities, a glorified transport van—into a mobile unit that could start resuscitation, manage airways, stabilize trauma, and make treatment decisions on the move.
Freedom House Ambulance Service is now widely recognized as a foundational chapter in the creation of American EMS: the first emergency medical service staffed by paramedics trained beyond basic first aid, and a program whose curriculum and equipment standards shaped national expectations for prehospital care. It is also, inseparably, a story about race and civic power. The service was created to address inequity—Black neighborhoods receiving inferior emergency response—and it was staffed overwhelmingly by Black Pittsburghers recruited from a labor market that had effectively written them off. The medical accomplishment is immense. The political afterlife is complicated. Both are essential to understanding what Freedom House was, and why its legacy still unsettles.
Before paramedics, before systems
In the mid-20th century, “emergency care” in much of the United States was a patchwork. Ambulances might be run by police departments, funeral homes, volunteer squads, or private operators with uneven training and minimal medical oversight. The focus was transportation, not intervention: get the patient to a hospital and hope the hospital can reverse whatever has happened. The weakness of that approach became harder to ignore as car culture intensified, cities grew more congested, and sudden cardiac death emerged as a highly visible killer.
A major national inflection point arrived in 1966 with the National Academy of Sciences and National Research Council report Accidental Death and Disability: The Neglected Disease of Modern Society, which described emergency and trauma care as dangerously inadequate and helped spark reforms that eventually shaped modern EMS. The report’s significance is less about any single recommendation than about the lens it applied: accidental death and disability were being treated as inevitable when, in fact, many deaths could be prevented with better systems—communications, training, equipment, coordinated hospital response, and rapid care delivered at the scene and en route.
Pittsburgh, like many industrial American cities, had reasons to confront this reality with particular urgency. It was a place of dense neighborhoods and steep topography, of factories and traffic, of occupational injury and street-level violence, of heart disease and asthma and the steady churn of emergencies that happen in any metropolis. It was also a city structured by segregation, redlining, and a long history of racial inequality that shaped everything from housing to healthcare access. If EMS was uneven nationally, it was especially uneven where political power was weakest.
The Hill District’s geography of need
The Hill District is often described in Pittsburgh history as both cultural engine and civic casualty. For decades it was a center of Black life—music, business, institutions, neighborhoods holding community even as the city’s policies extracted from them. By the 1960s, the Hill was also facing a familiar American pattern: disinvestment, crowding, and the destabilizing effects of “urban renewal,” which frequently meant the clearance of Black neighborhoods for development projects that served the wider city more than the residents displaced.
When residents talk about emergency response in that era, the details are practical. Who shows up when you call? How long does it take? What happens once they arrive? In many communities, the first responders were police officers with limited medical training or other improvised transport options, a system that could be particularly fraught in a neighborhood where police-community relations were tense. Even when intentions were good, the model was structurally weak. A police vehicle is not a clinic. A fast ride without treatment can be the difference between life and death.
Freedom House was conceived as a response to that lived reality: bring a medical service into the community that is both clinically sophisticated and socially credible. It would be staffed by people the neighborhood recognized—not as outside authority but as neighbors—and trained to a level that could compete with, and surpass, the care available elsewhere in the city.
Freedom House Enterprises and the logic of the War on Poverty
Freedom House Ambulance Service did not emerge from a hospital administrator’s office alone. It grew from the ecosystem of Freedom House Enterprises, a Hill District organization that addressed employment and community development in the context of the War on Poverty. The logic was radical in its simplicity: if the city treats a population as “unemployable,” build an institution that turns employment into infrastructure—work that benefits the community while expanding who gets to hold skilled, respected jobs.
In that framework, an ambulance service is not only a public health intervention; it is an economic strategy. It creates paid roles, requires training, demands professionalism, and produces measurable outcomes. Those outcomes can be lives saved, yes, but also a deeper civic outcome: the restoration of a community’s confidence that the city can deliver on its promises of equal protection and equal care.
Freedom House’s founding is often attributed to a partnership among community leaders and medical innovators, including Phil Hallen of the Maurice Falk Medical Fund, Dr. Peter Safar, and leadership within Freedom House Enterprises. Each brought something different: funding capacity and institutional access, medical vision, and a pipeline to recruit and support trainees from the Hill.
Peter Safar and the idea that medicine begins before the hospital
Dr. Peter Safar’s name appears in emergency medicine history for reasons that extend far beyond Pittsburgh. He is commonly described as a pioneer of resuscitation and CPR, and in many tellings of the Freedom House story, his push for advanced prehospital care is tied to both professional conviction and personal grief. Time’s account, for example, describes Safar creating modern paramedic training after losing his daughter to an asthma attack, a tragedy that sharpened his sense that lives can be lost in the gap between crisis and hospital care.
Whether one emphasizes the personal or the professional, the conceptual shift is the same: the “scene” is part of medicine. The ambulance is not merely transportation. The minutes before arrival—oxygenation, airway management, circulation, shock prevention—are a clinical arena that can be taught, standardized, and improved. Freedom House would become the proving ground for that idea.
The idea was controversial not because it lacked logic, but because it required a different type of worker. You would need people capable of learning complex procedures, making decisions under pressure, documenting care, and communicating with hospitals. And, in Pittsburgh’s plan, those people would largely be Black men and women recruited from a neighborhood the city had trained itself to view through deficit.
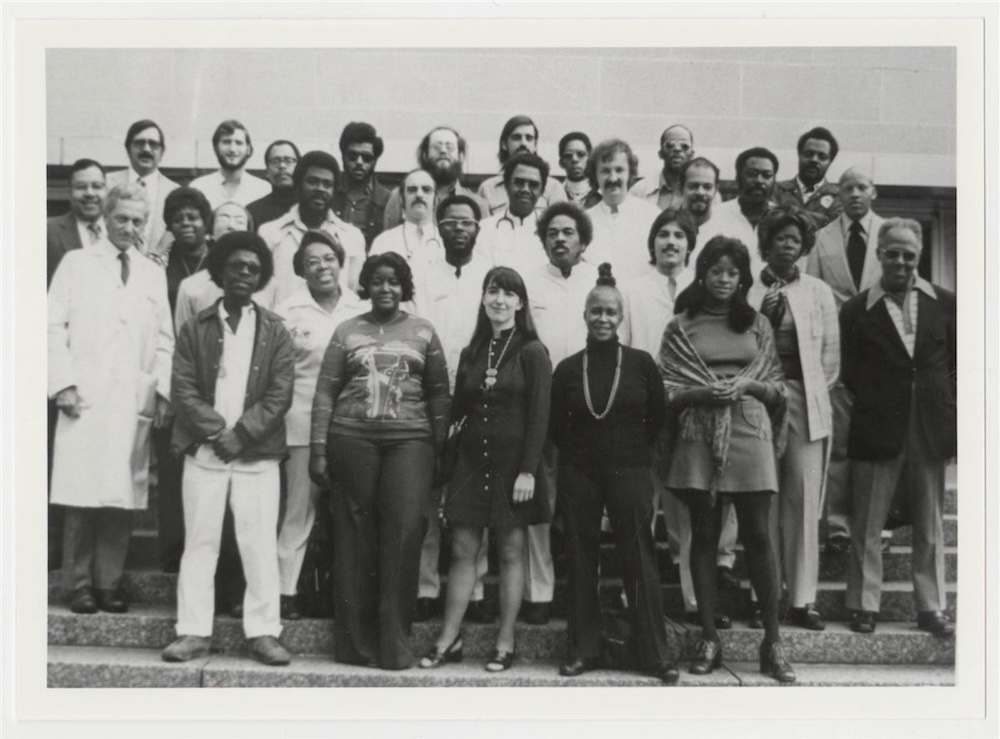
Nancy Caroline and the making of a curriculum
The Freedom House story has a second indispensable medical figure: Dr. Nancy Caroline, who served as medical director and helped shape the training that made Freedom House more than a well-meaning experiment. The Hill History Center account describes Caroline collaborating with Safar and Freedom House leadership to create a program called “Emergency Care in the Streets,” a 32-week course covering anatomy, physiology, CPR, advanced first aid, nursing, and even defensive driving.
The phrase “Emergency Care in the Streets” is important because it treats street medicine as a discipline, not an afterthought. It suggests that the environment—uncontrolled, chaotic, unpredictable—is not a reason to lower standards; it is a reason to raise them. A paramedic cannot request a quiet room. They cannot pause for the perfect lighting. They cannot ask a patient to wait until the hospital. They must work in cramped stairwells, in the back of a moving vehicle, in weather, in crowds, amid sirens and fear.
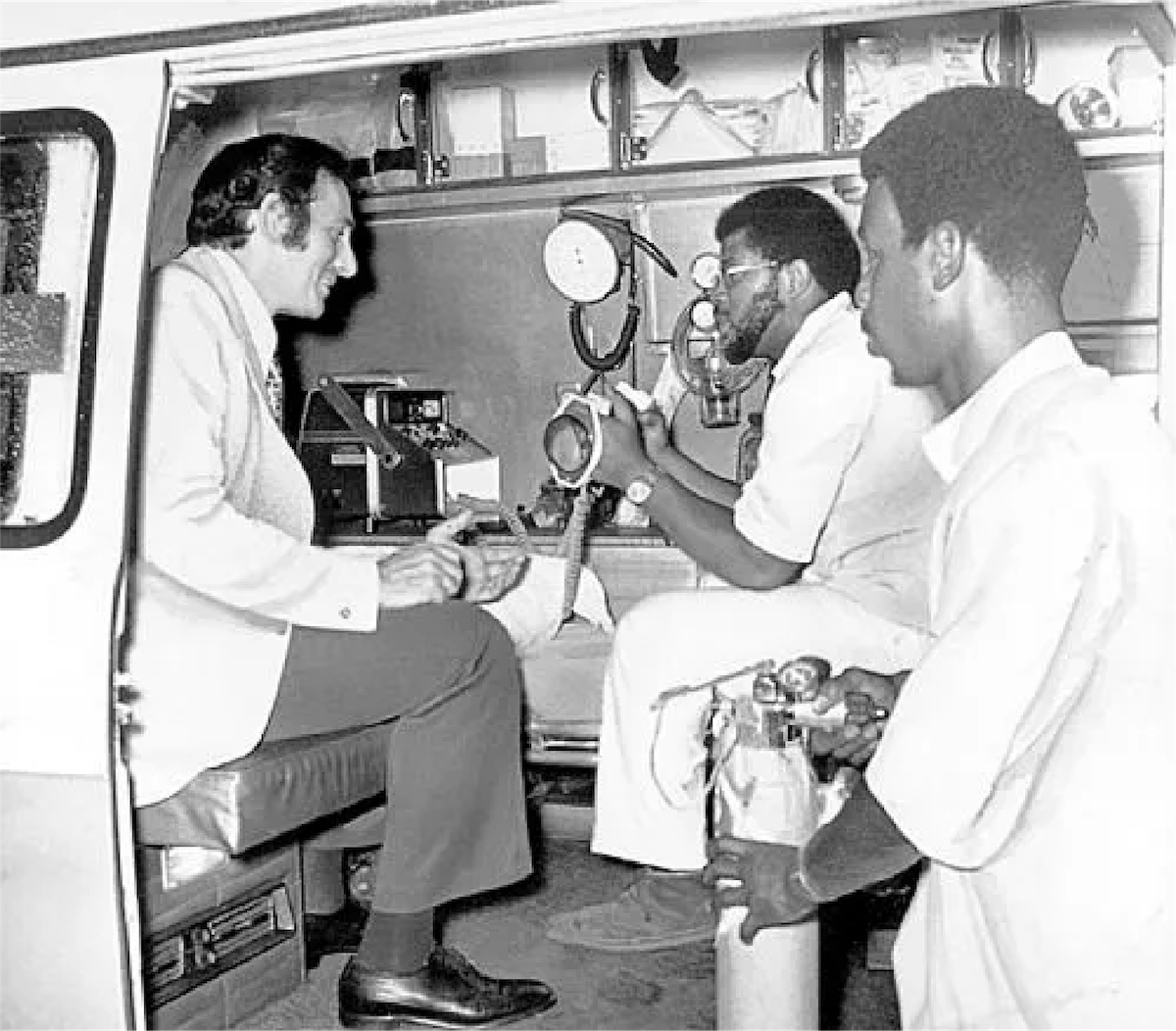
Training people to do that well requires more than courage. It requires a curriculum that can translate physiology into action and protocols into instinct. The University of Pittsburgh Health Sciences Library System notes that Freedom House training equipped paramedics with skills such as intubation and defibrillation—procedures not previously performed in out-of-hospital settings—underscoring how far beyond typical “ambulance driver” expectations the program aimed.
Over time, Caroline’s influence extended beyond Pittsburgh. She would become associated with EMS education more broadly, including the development of training resources that shaped the profession nationally—part of why Freedom House’s impact is understood not only through the stories of calls run, but through the structures of what paramedics are taught to know.


Recruitment: Turning “unemployable” into elite responders
One of the most startling aspects of Freedom House is the recruitment logic. The program sought trainees in a population that mainstream employers and institutions routinely rejected. The Journal of the History of Medicine and Allied Sciences article describes the program training “unemployable” Black citizens to provide state-of-the-art prehospital care, a framing that captures both the cruelty of the label and the audacity of the response.
The Atavist’s long narrative account adds texture: recruitment included Vietnam veterans and men with criminal records, reflecting how Freedom House drew from a community whose relationship to formal credentials and clean records was shaped by structural inequality as much as by individual history. This wasn’t a program that waited for the city’s ideal candidate. It created its own pipeline and built support around it.
That choice mattered clinically—because it expanded who could staff an EMS system—and politically, because it challenged the city’s implicit story about who could be trusted with life-and-death responsibility. In many American cities, the earliest paramedic cohorts were built from fire departments or other uniformed services already granted civic legitimacy. Pittsburgh’s Freedom House asked the city to grant legitimacy to people the city had habitually marginalized.
The early operations: “Send Freedom House”
Freedom House began in 1967 and started officially operating in 1968, initially serving the Hill District and later expanding to other parts of the city such as Downtown and Oakland. Residents learned quickly that the service brought something different: speed, competence, and advanced care.
In its first year, Freedom House handled thousands of calls. Multiple accounts cite figures in the range of roughly 5,800 runs and more than 4,600 transports, evidence of both the scale of need and the service’s centrality. In a neighborhood where emergency response had been a point of tension, that call volume also signals trust: people called because they believed help would come and would make a difference.
What did “advanced care” mean in that context? It meant bringing hospital logic into the field: assessing airways and breathing, managing circulation, treating shock, performing resuscitation, documenting vitals, and communicating with hospital staff in a structured way. It meant moving beyond “scoop and run” into interventions that bought time and prevented deterioration.
One reason the Freedom House story persists in memory is the drama of contrast. Before, people might be transported in vehicles not designed for medical care, without meaningful treatment. After, a team arrived trained to intervene. That shift is not abstract. For a patient in respiratory distress, airway management in minutes can be the difference between survival and death. For cardiac arrest, early CPR and defibrillation can be the difference between recovery and loss. Freedom House’s legacy is built from thousands of such moments.
Measuring success: Outcomes, data, and credibility
In medicine, credibility is often negotiated through numbers as much as narratives. Freedom House’s success was not only felt; it was documented. Time’s reporting highlights a 1972 study showing Freedom House paramedics provided accurate critical care far more often than police and volunteer services, a stark performance gap that reinforced what residents already knew.
Even without reciting every statistic, the existence of outcome comparisons is itself significant. It means Freedom House was not treated simply as charity or experiment. It was treated as a clinical system subject to evaluation. That evaluation made it harder to dismiss the service as symbolic—and, paradoxically, made its eventual dismantling more revealing. When an institution delivers superior results yet is still defunded or absorbed, the reasons are seldom clinical.
The Freedom House Wikipedia summary, drawing on multiple historical accounts, notes that Safar collected data suggesting the paramedics saved lives in the first year and achieved response times under ten minutes in most neighborhoods they served. Those metrics mattered in a city where response times and quality of care had been unevenly distributed. In emergency medicine, minutes are not just time; they are physiology.
Professional identity: Being excellent while being doubted
Freedom House’s medics did more than learn skills. They learned how to exist in a professional role that the city had not built with them in mind. They learned to speak the language of medicine, to present patients, to write reports, to communicate with emergency departments. Pitt Med’s “Send Freedom House!” narrative from 2004 captures a moment that illustrates this: a young paramedic preparing to present a patient to hospital staff with the structured confidence of a clinician—blood pressure, pulse, history—at a time when such sophistication in ambulance service was still “practically unheard of.”
That kind of professionalism is not only personal pride; it is strategic survival. In a racially stratified city, Black paramedics had to be unassailably competent because their competence would be tested more aggressively. They carried not only patients, but expectations. They represented a claim: that a Black-run, community-rooted service could be the standard, not the exception.
And they were doing this work in a neighborhood that would sometimes see them as both insiders and new authorities. The Atavist notes the complicated emotions among paramedics running the majority of their calls in the Hill: the pride of bringing care to their community and the frustration of being constrained by city policy. Freedom House was simultaneously a liberation—bringing advanced care to a neglected area—and a reminder of segregation’s boundaries, because the service’s reach was politically shaped.
The politics of control
If Freedom House were simply a success story, it would end with replication and expansion. In many ways, it did: the model of trained paramedics delivering advanced care in the field became foundational to EMS nationally, and Freedom House’s training and ambulance design standards are often cited as influential in the development of national norms.
But locally, success collided with a different impulse: municipal control. Cities often prefer services that are centralized, standardized, and directly managed by government. That preference is not inherently sinister. It can improve accountability and stability. Yet in Freedom House’s case, control politics were inseparable from race politics.
By the mid-1970s, Pittsburgh moved to create a citywide EMS system. Freedom House was defunded and closed in 1975 as the city set up its own emergency medical service. The medical model survived; the institution and much of its workforce did not.
The Journal of the History of Medicine and Allied Sciences article frames the Freedom House program as both medical and social experiment and explores the roles of Safar and Caroline, underscoring how leadership and institutional alignment shaped the program’s development—and implicitly, how vulnerable such a program can be when political winds shift. That vulnerability became reality when Pittsburgh decided to replace a community-rooted service with a city-run one.
Closure and displacement: What happens when the city takes the model
Freedom House closed on October 15, 1975. The closure is often described as administrative, but the human details reveal the deeper costs.
Accounts differ in emphasis, but a recurring theme is that the transition to the new city system did not preserve Freedom House’s crews, culture, or internal authority. The Wikipedia summary notes that the initial hires for the successor service were all white, and that when Freedom House paramedics were hired, their crews were broken up, exams were instituted covering material they had not been taught, and many were dismissed or reassigned to non-essential roles. Even allowing for the limitations of any single summary, the outline matches what broader journalism and scholarship have suggested: the dismantling was not merely structural; it was a re-sorting of power.
The Washington Post’s review of Kevin Hazzard’s American Sirens situates Freedom House in a segregated city shaped by redlining and “urban renewal,” and treats racism and politics as central to the program’s abandonment. That framing matters because it links the end of Freedom House to the same civic structures that made it necessary in the first place.
In 2026, as lawmakers and institutions seek belated recognition for Freedom House, public discussions still return to that unresolved question: how could a city dismantle a service that demonstrably saved lives and pioneered the future of emergency care? WESA’s reporting on proposed Congressional recognition explicitly notes that Kevin Hazzard and others cite racism in city government as a factor in the defunding.
Why erasure happens even when the evidence is strong
In the American civic imagination, innovation is supposed to be rewarded. But Freedom House sits at the intersection of innovation and legitimacy, and legitimacy is not granted equally.
One way to understand Freedom House’s erasure is to see it as a familiar cycle. A marginalized community creates a model that works. The wider system adopts the model. Then, rather than expanding the original institution and investing in its workforce, power restructures it into a form that feels more controllable and more aligned with existing hierarchies. The model remains; the originators are sidelined.
That cycle is easier to see in hindsight, but it was felt in real time by the people living it. Some former Freedom House paramedics went on to continued careers and leadership roles in EMS, but the broader pattern described in multiple accounts is one of lost opportunity—an institution that could have anchored a Black professional pipeline in emergency medicine, reduced disparities, and built durable community trust, instead treated as a temporary solution rather than a permanent civic asset.
The national impact: How Pittsburgh shaped the country’s response to crisis
If Pittsburgh’s local politics complicated Freedom House’s life, the national medical arc reveals its lasting significance. Freedom House helped prove that prehospital care could be professionalized, standardized, and made clinically sophisticated. It pushed the boundaries of what could be done outside hospitals, including procedures like intubation and defibrillation, and helped establish training expectations that later became common.
Smithsonian Magazine’s 2025 feature puts the point bluntly: Freedom House set the standard for emergency medical care and laid groundwork for the services available today, a reminder that the modern EMS experience—calling for help and expecting trained clinicians to arrive in an equipped ambulance—was not always a baseline assumption in American life.
This matters because EMS is one of the most intimate interfaces between a city and its residents. People do not encounter emergency responders as policy. They encounter them as an arrival at the worst moment of their lives. Trust in that arrival shapes whether people call early, whether they share information, whether they cooperate with care, whether they believe the city values their survival. Freedom House offered a model in which trust was not a public relations campaign but a design choice: recruit from the community, train intensively, treat people with dignity, deliver measurable clinical results.
Freedom House and the question of public safety beyond policing
In recent years, American debates about public safety have expanded beyond the binary of policing versus absence. Communities and policymakers have begun asking what it would mean to respond to crises—medical, behavioral health, substance use, mental health emergencies—with care rather than coercion. In that context, Freedom House appears not only as medical history but as civic blueprint.
WESA’s 2026 reporting describes the pre-Freedom House reality of police or funeral home drivers as responders, and it quotes former paramedic John Moon describing the profession’s essence: “We created the idea of bringing the emergency room to the person.” The line captures a philosophy that has renewed relevance. If the emergency room can be brought to the person, then a city can reimagine crisis response as healthcare infrastructure, not law enforcement.
ACEP Now’s 2026 reflection goes further, framing Freedom House’s legacy as a call to action and a reminder that “excellence and equity are linked”—a professional argument that the field of emergency medicine should not treat equity as separate from clinical innovation. Freedom House is a case study in that linkage: the push to deliver better care to a neglected Black neighborhood produced advances that benefited the whole country.
The long return: Documentaries, scholarship, and public recognition
For decades, Freedom House was better remembered by those who lived it than by the nation that inherited its innovations. That gap has narrowed in recent years thanks to journalism, scholarship, and public media.
The WQED documentary Freedom House Ambulance: The FIRST Responders has played a key role in reintroducing the story, emphasizing archival images, firsthand reflections, and the rise-and-fall arc that makes Freedom House both inspiring and infuriating. PBS has likewise framed the documentary as an exploration of how a Hill District service became the basis for paramedic training across the country.
Academic work has reinforced the story’s credibility and complexity. The 2019 Journal of the History of Medicine and Allied Sciences article describes extensive archival research—newspapers, correspondence, university memoranda—and situates Freedom House within both medical development and racial politics. When a story is both morally resonant and empirically documentable, it becomes harder for institutions to dismiss it as myth.
In 2025, the American College of Surgeons’ bulletin highlighted how a Pennsylvania ambulance service helped lead to modern EMS, signaling institutional recognition from a major medical organization that trauma and emergency systems owe a debt to early prehospital innovations.
And in early 2026, recognition has entered the political arena. WESA reported that U.S. Rep. Summer Lee planned to introduce bipartisan legislation to award a Congressional Gold Medal to Freedom House, framing it as the nation’s first professional emergency-medicine unit and emphasizing its Hill District roots. Rep. Lee’s official press release similarly describes the effort to honor Freedom House for its service and contributions to EMS.
Local institutions have moved as well. Axios reported in February 2026 that the Heinz History Center was spotlighting Freedom House through images and artifacts as part of an exhibit on Pittsburgh innovation, noting renewed awareness driven by the WQED documentary and references in popular culture.
Freedom House 2.0 and the question of repair
Recognition is not the same as repair, but it can create pressure for it. In Pittsburgh, recent initiatives suggest an attempt to translate commemoration into pipeline.
WESA reported in 2024 that Pittsburgh announced a new EMT training program tied to Black History Month celebrations and inspired by Freedom House, with the city’s EMS leadership connecting the present to the past. The point is not nostalgia. It is workforce development, community investment, and a public acknowledgement that the profession’s roots in Pittsburgh are inseparable from the Hill District and the Black medics who made modern EMS possible.
In 2025 and 2026, local and regional coverage has continued to note new cohorts and renewed public attention, including stories about how Freedom House is being honored and re-taught as part of a living civic narrative rather than a closed chapter. That matters because Freedom House’s original injustice was not only the closure; it was the failure to preserve an institution that could have anchored ongoing opportunity.
The most meaningful legacy is often the one that changes who gets to participate. If Freedom House’s story becomes merely a plaque or a documentary clip, the city risks repeating the original pattern: extracting inspiration without building infrastructure. But if the story becomes a blueprint for training programs, recruitment pipelines, and community-rooted EMS strategies, then remembrance can become a kind of delayed justice.
The ethical spine of the story
Writing about Freedom House demands an ethical approach because the story is often told in a way that can slip into easy heroism. Heroism is real here, but it is also incomplete. The medics were heroic because the system demanded they be heroic. They worked in an era when their professionalism was questioned, their community underserved, and their institutional survival precarious. The story’s triumph is inseparable from its critique: the United States can produce extraordinary innovation in marginalized communities and still deny those communities durable control over what they build.
There is also an ethical tension in the way Freedom House is sometimes framed as “first.” EMS history includes multiple local innovations across the country, including programs often cited in Seattle/King County and elsewhere. Freedom House’s distinct claim, supported across many accounts, is its early role as a fully trained paramedic-staffed service with advanced clinical standards and its influence on national training and ambulance design. The point is not to flatten other histories, but to accurately name what Freedom House did that was exceptional—and why it was exceptional that it came from the Hill.
What “Send Freedom House” means now
If you listen closely to the way Freedom House is discussed today—in documentaries, scholarship, policy conversations, and the memories of those who served—you hear two stories traveling together.
The first is a story of medical transformation. It is the story of an ambulance becoming a mobile treatment space; of dispatch and training and protocols turning chaos into care; of prehospital intervention becoming a profession. It is the story of outcomes that can be measured and practices that can be taught and replicated. That is the story modern EMS likes to tell about itself, because it is a story of progress.
The second is a story of American power. It is the story of a Black community building a model that worked, and of a city absorbing the model while destabilizing the institution and people who pioneered it. It is the story of how innovation does not automatically produce equity, and how “professionalization” can sometimes function as a euphemism for re-centralizing authority away from communities that proved they could lead.
To hold both stories at once is to see Freedom House clearly. The dispatch call—Send Freedom House—was a request for life-saving care. It was also, whether residents said it consciously or not, a vote for a different kind of city: one where medical competence and community trust were treated as inseparable; one where the Hill District was not a place to be managed but a place to be invested in; one where Black residents were not merely patients but practitioners and pioneers.
That is why the Freedom House story keeps coming back. It is not just a piece of Pittsburgh history. It is a question posed to every American city that has ever benefited from the labor and invention of marginalized communities: when the people you’ve overlooked build the future anyway, what do you owe them besides applause?
More great stories
Harlem, in Bronze
February 28, 2026
No Comments
Sojourner Truth, Detroit, and the Price of a Key
February 28, 2026
No Comments